eBook - ePub
Robotic Assistive Technologies
Principles and Practice
- 382 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Robotic Assistive Technologies
Principles and Practice
About this book
This book contains a comprehensive overview of all current uses of robots in rehabilitation. The underlying principles in each application are provided. This is followed by a critical review of the technology available, of the utilization protocols, and of user studies, outcomes, and clinical evidence, if existing. Ethical and social implications of robot use are also discussed. The reader will have an in depth view of rehabilitation robots, from principles to practice.
Trusted by 375,005 students
Access to over 1 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Fundamentals of Robotic Assistive Technologies
Contents
Assistive Technology
Robots
Safety of Service Robots
Technology Readiness Scale
Summary
References
Learning Objectives
After completing this chapter, readers will be able to
- Describe the different conceptualizations of disability.
- Define assistive technology.
- Describe the Human Activity Assistive Technology (HAAT) model.
- Define and classify a robot.
- Justify the use of robots in rehabilitation.
- Discuss the current international safety standards for robotic assistive technologies.
- List some of the challenges of the rehabilitation robotics market.
- Explain the goal of a Technology Readiness Levels scale.
Assistive Technology
The term rehabilitation in this book refers to the entire process aimed at enabling people with disabilities “to reach and maintain their optimal physical, sensory, intellectual, psychological and social functional levels” (World Health Organization [WHO] 2016a). The concept of disability has evolved through the years. It was first seen as a purely medical problem: a disease led to an impairment (abnormality of a body structure or appearance or malfunction of an organ or system), which led to a disability (limitation to functional performance and activity of the individual), which in turn led to a handicap (disadvantage experienced by the individual as a result of the individual’s disability and impairments) (WHO 1980). Focus was on the impairment that prevented an individual from performing. The social model by Oliver (1990) completely changed the perspective focusing on the barriers erected by society that hinder full participation of people with disabilities. Under this model, it is the society that disables people; disability is not something intrinsic to the individual.
In 2001, WHO adopted the International Classification of Functioning, Disability, and Health (ICF) that integrates the medical and the social models of disability into a biopsychosocial model (WHO 2001). In the ICF, disability covers impairments, activity limitations, and participation restrictions. Impairments are related to problems in the individual’s body function or structure; activity limitations refer to the difficulties encountered by an individual in executing a task or action; and participation restrictions encompass problems experienced by an individual in involvement in life situations (WHO 2001). Disability reflects the negative aspects of the interaction between the individual’s health condition and contextual (environmental and personal) factors. Equally relevant in ICF is the concept of functionality covering body functions, body structures, activities, and participation and denoting the positive or neutral aspects of the interaction between the individual’s health condition and that individual’s contextual factors (WHO 2001). Figure 1.1 illustrates the ICF conceptualization of disability as multidimensional and interactive, resulting from the dynamic interaction between body functions and structures, activities, and participation, influenced by the individual’s health condition and environmental and personal factors. Despite this paradigm shift, the medical perspective is still omnipresent in statements like “he can’t read the newspaper because he’s blind.”
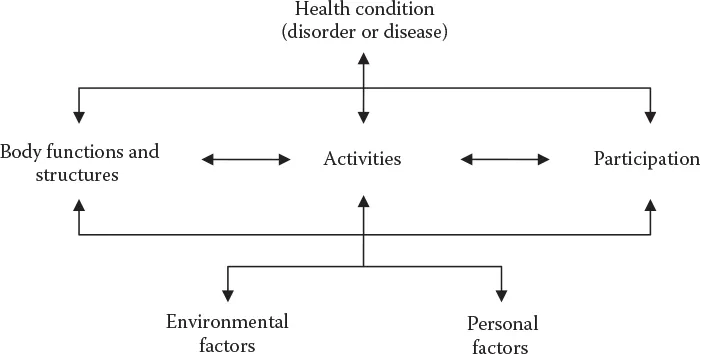
Figure 1.1 Interactions between the components of ICF. (From World Health Organization. International Classification of Functioning, Disability and Health (ICF). Geneva: WHO, 2001.)
A major goal in rehabilitation is allowing independence and self-determination for people with disabilities. To bridge the gap between the capabilities of an individual with disabilities and the requirements of an activity the person wants to perform, one or a combination of the following four strategies can be used (EUSTAT 1999): (1) receive training to improve the individual’s capabilities; (2) change the environment to reduce the requirements of the activity; (3) use adequate assistive technology to perform the activity; or (4) have a personal helper do or help with the activity.
Assistive Technology means technology designed to be utilized in an assistive technology device or assistive technology service. Note that the term technology is used here as “the practical application of knowledge especially in a particular area” (“technology,” Merriam-Webster OnLine) and not as a machine or piece of equipment that is created by technology. The latter is designated here by the term technology device. According to the U.S. Assistive Technology Act of 2004, as amended (Public Law 108-364 2004, 118 STAT. 1709–1710):
The term “assistive technology device” means any item, piece of equipment, or product system, whether acquired commercially, modified, or customized, that is used to increase, maintain, or improve functional capabilities of individuals with disabilities.
The term “assistive technology service” means any service that directly assists an individual with a disability in the selection, acquisition, or use of an assistive technology device. Such term includes
(A) The evaluation of the assistive technology needs of an individual with a disability, including a functional evaluation of the impact of the provision of appropriate assistive technology and appropriate services to the individual in the customary environment of the individual;
(B) Services consisting of purchasing, leasing, or otherwise providing for the acquisition of assistive technology devices by individuals with disabilities;
(C) Services consisting of selecting, designing, fitting, customizing, adapting, applying, maintaining, repairing, or replacing assistive technology devices;
(D) Coordination and use of necessary therapies, interventions, or services with assistive technology devices, such as therapies, interventions, or services associated with education and rehabilitation plans and programs;
(E) Training or technical assistance for an individual with disabilities, or, where appropriate, the family members, guardians, advocates, or authorized representatives of such an individual; and
(F) Training or technical assistance for professionals (including individuals providing education and rehabilitation services), employers, or other individuals who provide services to, employ, or are otherwise substantially involved in the major life functions of individuals with disabilities.
In other words, assistive technology refers to technology that helps an individual carry out a functional activity, taking part in the person’s daily life. Technology used in rehabilitative or educational processes, respectively termed rehabilitative or educational technology, is outside the scope of this book.
Several models have been proposed conceptualizing assistive technology. Examples include the HEART (Horizontal European Activities in Rehabilitation Technology) model (Azevedo et al. 1994); the HAAT model (Cook and Polgar 2015); the Enders (1999) model; and the dynamic circles of human activities model by Azevedo (2006). Common to all models is the focus on the activity that the individual with disabilities wants to perform, including the assistive technology necessary to perform the activity and the context in which the activity takes place.
For a comprehensive discussion of the HAAT model, please refer to the work of Cook and Polgar (2015). A short description is provided here. The HAAT model has four components: the human, the activity, the assistive technology, and the context that frames the first three factors. It models an assistive technology system representing a person with a disability doing an activity using an assistive technology within a context.
The activity defines the overall goal of the assistive technology system. Activities can be categorized into activities of daily living (e.g., dressing, hygiene, eating, communication); work and productive activities (including home management, educational, vocational, and care-of-others activities); and leisure activities (Canadian Association of Occupational Therapists 2002). The same activity for different persons or in different contexts can be placed in a different category. For example, one person may cook for work while another cooks to relax. Or, the same person may drive a car differently in the role of a professional driver compared to when travelling with the family. The selection of an assistive technology depends on a deep understanding of the activity. Important questions to be addressed include the following: Which skills and abilities does it require from the person? What is the meaning of the activity to the person? In which contexts is the activity performed?
The human component of the HAAT model refers to the person with disabilities with his or her physical and cognitive abilities and emotional states. The human should be the central component in the assistive technology system. It is the person with disabilities who selects the activities he or she would like to perform and within which contexts. It is the gap between the capabilities of the person with disabilities and the requirements of the activity, along with the preferences of the person, that dictates the choice of an assistive technology. The subjective assessment of the person with disabilities plays a leading role when evaluating the effectiveness of an assistive technology system. Even more, persons with disabilities should be involved in the research and development of assistive technologies and not viewed solely as the recipients of the technologies.
The context in which activities are performed includes physical, social, cultural, and institutional facets. Contexts may enable or hinder the use of assistive technology. The physical characteristics of the natural or built environment in which a given activity will be performed have a direct influence on the assistive technology that can be used. For example, they determine the maximum width that a wheelchair can have to be able to cross doorways, or they determine the reflective properties of a display that is supposed to be used under natural light. But, social (referring to those persons who interact with the assistive technology user), cultural, and institutional environments are also of paramount importance when considering assistive technology. Persons with disabilities often report that attitudes of others are frequently more disabling than physical barriers. The use of assistive technology can accentuate disability and contribute to stigmatization (see Chapter 10). Success of assistive technology use depends also on how knowledgeable of assistive technology the persons interacting with the individuals with disabilities are. Examples of cultural factors that affect assistive technology delivery are the degree of importance attributed to physical appearance and to independence, typical coping strategies, and typical roles of a person in society. Finally, funding policies and regulations, accessibility legislation, and standards for product design are examples of factors in the institutional context that affect assistive technology.
The assistive technology component in the HAAT model is what enables the human to perform the activity within a given context. Assistive technology devices can be conceptually divided into functional blocks that represent the information flow and the interaction between the device and the other components of the model (Figure 1.2). The human-technology interface encompasses the interactions from the human to the technology and from the technology to the human. It thus includes positioning devices that enable a person to maintain a functional position to interact with the technology; control interfaces that allow a person to control the technology (e.g., joysticks, keyboards, switches); and displays (visual, auditory, or tactile) that relay information to the user. Chapter 2 discusses the human-technology interface in robotic assistive technologies. The environmental interface is responsible for gathering environmental information necessary for the functioning of the technology. For example, cameras can be used for a socially assistive robot (SAR) to perceive the user affect (cf. Chapter 8). The processor block receives and processes the user commands and the ...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- Acknowledgments
- Editorial Board
- Contributors
- 1. Fundamentals of Robotic Assistive Technologies
- 2. Human–Robot Interaction for Rehabilitation Robots
- 3. Assistive Robotic Manipulators
- 4. Upper and Lower Limb Robotic Prostheses
- 5. Smart Wheelchairs for Assessment and Mobility
- 6. Exoskeletons as an Assistive Technology for Mobility and Manipulation
- 7. Robotic Systems for Augmentative Manipulation to Promote Cognitive Development, Play, and Education
- 8. Social Assistive Robots for Children with Complex Disabilities
- 9. Robots Supporting Care for Elderly People
- 10. Ethical and Social Implications of the Use of Robots in Rehabilitation Practice
- Glossary
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Robotic Assistive Technologies by Pedro Encarnação, Albert Cook, Pedro Encarnação,Albert Cook in PDF and/or ePUB format, as well as other popular books in Medicine & Biotechnology in Medicine. We have over one million books available in our catalogue for you to explore.